In rare and orphan diseases, the patient journey is often described as a “diagnostic odyssey.” But that phrase can unintentionally oversimplify what is, in reality, a fragmented, non-linear progression across providers, institutions, and systems. Patients may see multiple specialists, receive conflicting information, and experience significant delays before reaching clarity.
Traditional journey maps tend to reduce this complexity into milestones: symptom onset, diagnosis, treatment initiation, and ongoing care. While helpful at a high level, this linear framing often obscures the true points of friction. In rare disease, barriers are rarely just patient-level challenges. They are frequently embedded within systems of care.
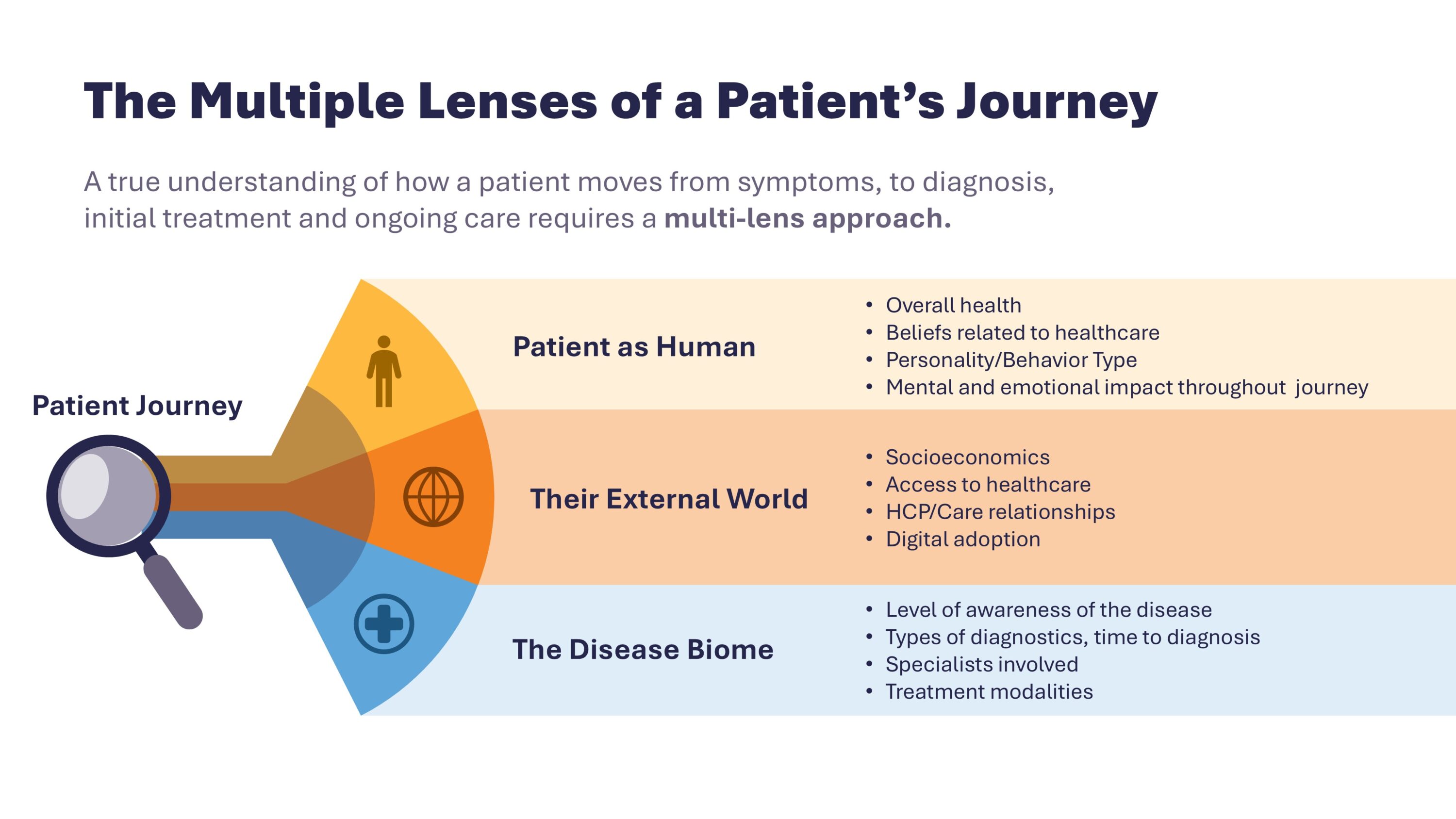
To truly understand and improve the rare disease journey, it must be examined through multiple lenses: the patient as a human, their external world, and the disease biome.
Lens One: Patient as Human
At the center of any rare disease journey is a person, not a pathway.
This lens goes beyond documenting experience. It incorporates behavioral science to uncover the underlying cognitive, emotional, and contextual drivers that shape how patients navigate care. Health beliefs, trust in the healthcare system, coping styles, and prior experiences all influence how individuals interpret symptoms, evaluate information, and engage with treatment options.
Two patients with the same condition may move through similar clinical steps, yet respond very differently. One may actively self-advocate, research extensively, and seek second opinions. Another may defer to providers, struggle with uncertainty, or disengage after repeated setbacks. Emotional burden, stigma, and mental fatigue can meaningfully affect adherence and long-term engagement.
In rare disease, advocacy is often not optional. Patients and caregivers frequently become coordinators of care, educators of providers, and navigators of insurance and access hurdles.
Understanding these behavioral and emotional dynamics is essential for identifying what truly drives decision-making and engagement across the journey.
Lens Two: Their External World
Even the most informed and proactive patient operates within a broader system.
This lens focuses on the structural and environmental factors that shape the journey: access to specialists, referral pathways, socioeconomic realities, insurance constraints, and variability in provider awareness. In rare disease, patients may encounter fragmented care across multiple specialties, with limited coordination between providers.
What appears to be a patient barrier is often a systems barrier. Delays may stem from referral bottlenecks. Miscommunication may arise from siloed care teams. Education gaps may persist even at the specialist level, particularly outside centers of excellence.
Digital adoption and access to online communities can also influence how patients seek information and advocate for themselves, but these factors are not universally distributed.
Mapping the external world reveals where infrastructure and communication breakdowns create friction points that directly impact outcomes.
Lens Three: The Disease Biome
The disease biome provides the foundational clinical context.
This includes symptom presentation patterns, diagnostic complexity, the range of specialists involved, and available treatment modalities. In rare and orphan diseases, symptom variability and low prevalence can make recognition and diagnosis particularly challenging.
Most journey mapping efforts start and stop at the clinical layer – documenting pathways and key decision points from both the patient and healthcare provider perspective. While this view is essential, it remains insufficient on its own. The same disease biome can produce very different lived experiences depending on patients’ behavioral drivers and the realities of the system in which care is delivered.
Integrating the Lenses
The true value of patient journey mapping in rare disease emerges when these three lenses are integrated.
Layering behavioral science insights onto systemic realities and clinical context allows organizations to identify where interventions will have the greatest impact. This integrated view can inform clinical development strategy, highlight diagnostic education needs, shape patient and provider messaging, and guide the design of support programs aligned with real-world friction.
It can also strengthen trial planning by revealing engagement barriers, support gaps, and lived experience factors that influence participation and retention.
Rare disease journeys cannot be flattened into timelines. They must be interrogated across human, systemic, and biological dimensions. A multi-lens approach transforms complexity into clarity and insight into action.
Authors
Marilisa Beatty, MA
Qualitative Research, VP
Marilisa is a seasoned qualitative researcher with over 16 years in global healthcare research. She has shaped strategies for top pharmaceutical brands and emerging biotech firms. She is known for her problem-solving skills, innovative research methods, and personable rapport with healthcare professionals, patients, and caregivers.
Ellen J. Gordon, PhD
Client Strategy & Growth, SVP
Ellen is an accomplished senior insights professional. Her understanding of client needs spans R&D, digital health, and commercial strategy, positioning her as a trusted partner for life science companies. Ellen is passionate about using emerging technology such as genAI to enhance market research. Ellen holds a PhD from the University of Michigan.
